- Use the patient's admission / initial values — the score was derived from labs at presentation, not later peaks or nadirs.
- Select age band and sex, then enter the initial creatinine, calcium, CPK, phosphate, and bicarbonate (raw values; the tool bins them for you).
- Choose the cause of rhabdomyolysis: the lower-risk causes (seizures, syncope, exercise, statin, or myositis) score 0; any other cause scores 3.
- The total McMahon Score and its risk category update automatically. Score < 6 → low risk; ≥ 6 → elevated risk that rises steeply (≥ 10 very high).
All computation runs in your browser; no values are stored or transmitted.
When to Use
Use the McMahon Score at presentation in a patient with confirmed or suspected rhabdomyolysis to estimate the risk of the composite outcome of death or AKI requiring renal replacement therapy. It converts the admission age, sex, chemistry, and cause into a single risk stratum that helps decide intensity of monitoring, fluid management, and whether early nephrology or ICU involvement is warranted. A score below 6 reassures that RRT is unlikely; a score of 6 or higher should prompt close monitoring and aggressive management.
Appropriate population
Adults presenting with rhabdomyolysis — from trauma or crush injury, prolonged immobilization, drugs and toxins, seizures, extreme exertion, statin myopathy, or myositis — in whom admission labs (creatinine, calcium, CPK, phosphate, bicarbonate) are available. Best applied to the initial presentation when triage decisions are being made.
When NOT to rely on it
The score is a risk-prediction aid, not a treatment threshold. It does not replace clinical judgment or serial monitoring, and aggressive IV crystalloid resuscitation remains the cornerstone of management regardless of the score. It was derived and validated for the composite of death or RRT-requiring AKI; do not use it to predict other outcomes or to withhold fluids or nephrology input in a deteriorating patient. Re-assess clinically as labs evolve.
Pearls & Pitfalls
A score < 6 is reassuring
In the derivation cohort, patients with a McMahon Score below 6 had a low (~3%) risk of the composite of death or RRT-requiring AKI. These patients generally do not need dialysis and can usually be managed with aggressive IV fluids and monitoring. The score is most useful precisely for identifying this large low-risk group who can be spared escalation.
The multivariable score beats CK alone
Peak or admission CK correlates only weakly with the need for RRT — many patients with very high CK never require dialysis, and some with modest CK do. The McMahon Score performs better because it integrates renal function, electrolytes, acid–base status, and the cause of injury, not just muscle enzyme release. Use the composite score rather than CPK in isolation for risk stratification.
Caveats
(1) The score predicts the composite of death or RRT-requiring AKI — it does not by itself tell you which. (2) Use admission/initial labs; substituting later peaks or treated values changes the bins and the meaning. (3) A high score never substitutes for treatment — aggressive IV crystalloid remains the cornerstone regardless of score. (4) Risk rises steeply with the score; a value ≥ 10 marks a very-high-risk patient in whom early nephrology and ICU involvement should be anticipated.
Why Use It
Not every patient with rhabdomyolysis develops kidney failure, and CK level alone is a poor guide to who will. The McMahon Score was derived to fill that gap: from a large cohort of patients admitted with rhabdomyolysis, it identifies the few admission variables that independently predict the composite of death or AKI requiring renal replacement therapy, and combines them into a simple additive score. For the nephrologist and intensivist this converts a vague clinical impression into a defensible risk estimate at the moment triage decisions are made — which patients can be managed on the ward with fluids, and which need early nephrology and ICU involvement, closer monitoring, and anticipation of dialysis. It does not change the fundamentals of management (aggressive crystalloid resuscitation), but it sharpens where attention and resources should be concentrated.
McMahon Score — Rhabdomyolysis AKI / RRT Risk
Select the age band and sex, enter the patient's initial creatinine, calcium, CPK, phosphate, and bicarbonate, and choose the cause. The total McMahon Score and risk category update automatically once age and sex are chosen; blank labs are treated as 0 points until entered.
⚕ McMahon GM, Zeng X, Waikar SS. JAMA Intern Med. 2013;173(19):1821–1828. The McMahon Score estimates the risk of the composite of death or AKI requiring renal replacement therapy in rhabdomyolysis from admission/initial values. It is a risk-prediction aid, not a treatment threshold: aggressive IV crystalloid resuscitation remains the cornerstone regardless of score. For licensed clinicians; not a substitute for individualized assessment.
Next Steps
Use the risk category to set monitoring intensity and the threshold for nephrology / ICU involvement — never to defer fluid resuscitation.
- Score < 6 (low risk): risk of RRT-requiring AKI or death is low (~3%). Manage with aggressive IV crystalloid, monitor urine output, creatinine, potassium, and CK trend; most patients do not require dialysis.
- Score 6–9 (elevated risk): anticipate AKI; intensify monitoring, ensure adequate volume resuscitation, watch potassium and acid–base closely, and involve nephrology early.
- Score ≥ 10 (very high risk): high probability of AKI requiring RRT or death. Manage in an ICU-level setting, involve nephrology promptly, and anticipate the need for renal replacement therapy.
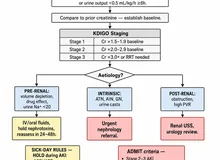
- Stage the kidney injury with KDIGO AKI staging and use FENa / FEUrea to help characterize the injury as labs evolve.
Evidence & References
Variable scoring
| Variable | Category → points |
|---|---|
| Age (years) | ≤ 50 → 0 · 51–70 → 1.5 · 71–80 → 2.5 · > 80 → 3 |
| Sex | Female → 1 · Male → 0 |
| Initial creatinine (mg/dL) | < 1.4 → 0 · 1.4–2.2 → 1.5 · > 2.2 → 3 |
| Initial calcium (mg/dL) | < 7.5 → 2 · otherwise → 0 |
| Initial CPK (U/L) | > 40,000 → 2 · otherwise → 0 |
| Initial phosphate (mg/dL) | < 4.0 → 0 · 4.0–5.4 → 1.5 · > 5.4 → 3 |
| Initial bicarbonate (mEq/L) | < 19 → 2 · otherwise → 0 |
| Cause | Seizures, syncope, exercise, statin, or myositis → 0 · other → 3 |
Interpretation of the total score
| Total score | Interpretation |
|---|---|
| < 6 | Low risk — risk of death or RRT-requiring AKI ~3%; RRT rarely needed, fluid management usually sufficient |
| 6–9 | Elevated risk — anticipate AKI; intensify monitoring and involve nephrology early |
| ≥ 10 | Very high risk — high probability of AKI requiring RRT or death; ICU-level care, anticipate dialysis |
McMahon and colleagues derived this additive risk score from a large cohort of patients admitted with rhabdomyolysis, selecting the admission variables that independently predicted the composite of in-hospital death or AKI requiring renal replacement therapy. The risk of the outcome rises steeply as the total score increases.
References
- McMahon GM, Zeng X, Waikar SS. A risk prediction score for kidney failure or mortality in rhabdomyolysis. JAMA Intern Med. 2013;173(19):1821–1828.
- Bosch X, Poch E, Grau JM. Rhabdomyolysis and acute kidney injury. N Engl J Med. 2009;361(1):62–72.
- Petejova N, Martinek A. Acute kidney injury due to rhabdomyolysis and renal replacement therapy: a critical review. Crit Care. 2014;18(3):224.