- Select your creatinine units (mg/dL or μmol/L) and your urea-nitrogen units (BUN mg/dL or Urea mmol/L) using the toggle buttons at the top of the calculator panel. The creatinine toggle updates all four creatinine label/placeholder fields simultaneously.
- Enter serum sodium and urine sodium from a spot urine collection (any voided urine, not a 24-hour collection).
- Enter serum creatinine and urine creatinine from the same paired draw.
- Optionally, enter serum BUN and urine BUN (from the same spot urine) to compute FeUrea. This is the preferred test when the patient has received any diuretic within the past 24–48 hours.
- Click Calculate. Results appear immediately with a color-coded interpretation: green = prerenal, amber = borderline, red = intrinsic AKI.
All computation runs in your browser; no values are stored or transmitted.
When to Use
Use FeNa when evaluating a patient with acute kidney injury (AKI) to distinguish volume-depleted prerenal azotemia (where the kidneys are appropriately retaining sodium) from intrinsic renal parenchymal injury (where the tubules have lost the ability to reabsorb sodium and reabsorb urea). Use FeUrea instead when the patient is receiving loop or thiazide diuretics, because diuretics directly force urinary sodium excretion and render FeNa falsely elevated.
Appropriate use
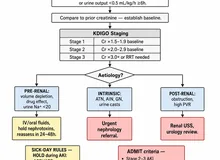
Adults with AKI (KDIGO: serum creatinine rise ≥ 0.3 mg/dL within 48 h, or ×1.5 baseline within 7 days) where the aetiology is uncertain between prerenal and intrinsic causes. A concurrent spot urine sodium and creatinine is required; a paired serum sodium and creatinine completes the test. BUN values are optional but needed to compute FeUrea.
When NOT to rely on FeNa
FeNa is unreliable (falsely elevated in prerenal, falsely normal in intrinsic) in the following situations: any diuretic use within the past 24–48 hours; acute glomerulonephritis (tubular function intact, low FeNa despite intrinsic injury); myoglobinuria and contrast nephropathy (both can give FeNa < 1% with true intrinsic AKI); and severe metabolic alkalosis. In these situations, use FeUrea if BUN values are available.
Pearls & Pitfalls
Use FeUrea when diuretics are present
Loop diuretics (furosemide) and thiazides directly block tubular sodium reabsorption, causing elevated urinary sodium regardless of volume status. FeNa of 2–4% may be seen in a genuinely volume-depleted patient who just received furosemide. In that context, FeUrea < 35% still correctly identifies preserved tubular function and a prerenal state, because urea reabsorption is driven by ADH-mediated water reabsorption, not the sodium transporters that diuretics block.
Pair with urine sediment and BUN/Cr ratio
FeNa and FeUrea are most powerful when combined with urine microscopy. Muddy-brown granular casts (ATN), eosinophiluria with white cell casts (AIN), and dysmorphic red cells with red cell casts (GN) each point toward specific intrinsic diagnoses. A BUN-to-creatinine ratio > 20 supports enhanced tubular urea reabsorption, consistent with prerenal physiology. A ratio < 10 is consistent with ATN or a high protein-catabolic state.
Pitfalls
(1) Myoglobinuria (rhabdomyolysis), contrast nephropathy, and acute GN can each produce FeNa < 1% despite intrinsic AKI — do not anchor on a low FeNa without checking CPK, contrast history, and urine sediment. (2) Chronic kidney disease blunts tubular sodium-reabsorption reserve; patients with CKD may have FeNa > 1% at their new steady state even without AKI. (3) Osmotic diuresis (high glucose, mannitol) increases urinary urea and makes FeUrea less reliable. (4) Neither test works when urine output is anuric (< 50 mL/day) — no sample, no test.
Why Use It
The distinction between prerenal and intrinsic AKI drives the entire management pathway. In prerenal AKI, volume resuscitation and removal of offending agents (NSAIDs, ACE inhibitors, ARBs) typically restores kidney function within 24–48 hours without the need for dialysis. In intrinsic AKI — particularly acute tubular necrosis (ATN) or acute interstitial nephritis (AIN) — the kidney tubules are structurally injured, fluid administration may cause volume overload without benefit, and the causative agent (contrast, aminoglycoside, proton pump inhibitor, beta-lactam) must be identified and stopped. Misclassification exposes the patient either to ongoing ischemia (from untreated hypovolemia) or to pulmonary edema (from volume loading ATN). FeNa and FeUrea provide a quantitative threshold to guide this critical decision at the bedside from a simple spot urine sample.
FeNa / FeUrea Calculator — Prerenal vs Intrinsic AKI
Enter serum and urine sodium and creatinine. BUN values are optional — add them if the patient is on diuretics to compute the more reliable FeUrea.
On diuretics? Add BUN/urea values below to calculate FeUrea (more reliable on diuretics):
⚕ FeNa and FeUrea are diagnostic aids, not standalone treatment triggers. Always correlate with history, physical examination, urine sediment, and clinical trajectory.
Next Steps
Use the result to support — not replace — clinical judgment.
- Interpret the value against the targets shown in the calculator and the Evidence section below, in the context of the full clinical picture.
- Trend serial measurements rather than acting on a single result; confirm abnormal or unexpected values before changing management.
- Apply the relevant KDIGO / specialty-guideline threshold and document the indication.
- Escalate or refer to nephrology when results are out of range, rapidly changing, or discordant with the clinical picture — and discuss the implications with the patient.
Evidence & References
Formula & Equations
| Test | Equation |
|---|---|
| FeNa (%) | (Urine Na⁺ × Serum Cr) / (Serum Na⁺ × Urine Cr) × 100 |
| FeUrea (%) | (Urine BUN × Serum Cr) / (Serum BUN × Urine Cr) × 100 |
Interpretation thresholds
| Value | FeNa interpretation | FeUrea interpretation |
|---|---|---|
| Low | < 1% → Prerenal (or GN / myoglobinuria) | < 35% → Prerenal azotemia |
| Borderline | 1–2% → Indeterminate; use FeUrea and clinical context | 35–50% → Indeterminate |
| High | > 2% → Intrinsic AKI (ATN, AIN, or GN with tubular injury) | > 50% → Intrinsic AKI (ATN) |
When creatinine units are μmol/L, the calculator converts to mg/dL (÷88.4) before applying the formula; display shows the input units. FeUrea is less affected by diuretics because tubular handling of urea is independent of the sodium transport pathways that diuretics block.
Evidence & References
FeNa was introduced by Espinel in 1976 as a simple bedside test to distinguish prerenal from intrinsic AKI, with the 1% threshold validated against urine culture and clinical criteria in a small cohort. The FeUrea method was proposed in 2002 by Carvounis et al. in a prospective study demonstrating its superiority over FeNa in patients receiving diuretics (FeUrea < 35% had a sensitivity of 90% for prerenal versus 48% for FeNa < 1% in that setting).
- Espinel CH. The FeNa test: use in the differential diagnosis of acute renal failure. JAMA. 1976;236(6):579–581.
- Carvounis CP, Nisar S, Guro-Razuman S. Significance of the fractional excretion of urea in the differential diagnosis of acute renal failure. Kidney Int. 2002;62(6):2223–2229.
- Miller TR, Anderson RJ, Linas SL, et al. Urinary diagnostic indices in acute renal failure: a prospective study. Ann Intern Med. 1978;89(1):47–50.