- Select your glucose units (mg/dL or mmol/L) and your urea-nitrogen units (BUN mg/dL or Urea mmol/L) using the unit toggle buttons. The calculator internally converts all values to mg/dL before applying the standard formula.
- Enter serum sodium (mEq/L), glucose, and BUN (or urea). These three values are sufficient to calculate the estimated osmolality.
- Optionally enter the lab-measured osmolality (mOsm/kg, from freezing-point depression). This field enables the osmolal gap calculation.
- Click Calculate (or values update automatically on input). Results appear with color coding: green = normal, amber/red = elevated gap requiring further evaluation.
All computation runs in your browser; no values are stored or transmitted.
When to Use
Use this tool in two distinct clinical scenarios: (1) to estimate the serum osmolality when a lab-measured value is not yet available, and (2) to compute the osmolal gap — the difference between the lab-measured osmolality and the calculated value — when you suspect an unmeasured osmole is present.
Key indications for the osmolal gap
- Unexplained altered mental status or metabolic acidosis — suspect toxic alcohol ingestion (methanol, ethylene glycol, isopropyl alcohol)
- Hyponatremia workup — to distinguish true hyponatremia from pseudohyponatremia (high lipids or protein) or isotonic hyponatremia (mannitol, glycine, sorbitol)
- Suspected mannitol toxicity in neurosurgical or renal patients receiving IV mannitol
- Evaluation of elevated anion gap metabolic acidosis when ethylene glycol or methanol poisoning is in the differential
When NOT to rely on a normal gap
A normal osmolal gap (< 10 mOsm/kg) does not exclude early toxic alcohol ingestion — it may be normal in the first few hours before significant metabolism has occurred, and in very small ingestions. If clinical suspicion is high (history of ingestion, anion gap acidosis, visual symptoms), send a toxic alcohol screen regardless of the gap.
Pearls & Pitfalls
Combine with anion gap for toxic alcohol workup
Early methanol or ethylene glycol ingestion (within 1–3 hours) will raise the osmolal gap before metabolism to toxic organic acids begins. As metabolism proceeds, the osmolal gap falls and the anion gap rises (from formate and glycolate accumulation). In late presentations, a normal osmolal gap with a high anion gap metabolic acidosis and normal lactate is highly suspicious for methanol or ethylene glycol. Run both gaps together at every stage.
Hyponatremia workup: estimated vs measured osmolality
In isotonic and hypertonic hyponatremia (mannitol, sorbitol from TURP, hyperglycemia), the calculated osmolality will be normal or high while the serum sodium is low. An osmolal gap in hyponatremia that cannot be explained by glucose, mannitol, or lipid infusion should prompt a toxicology screen. In pseudohyponatremia from extreme hyperlipidemia or paraproteinemia, the measured osmolality is normal (correcting the gap back to zero) while the flame-photometry sodium reads falsely low.
Pitfalls
(1) A normal osmolal gap does not exclude toxic alcohol ingestion in the early phase — always send a serum toxic alcohol level when ingestion is plausible. (2) Ethanol itself contributes to the osmolal gap — a patient who is intoxicated will have a gap from ethanol alone (~22 mOsm/kg per 100 mg/dL ethanol). Subtract the ethanol contribution (ethanol mg/dL ÷ 4.6) to assess whether an additional osmole is present. (3) The formula assumes conventional (freezing-point) osmometry — vapor-pressure osmometry is not equivalent and will give a different gap. (4) Very high BUN or glucose values normally raise the calculated osmolality; be sure the "gap" is not simply from miscategorized hyperglycemia or severe uremia.
Why Use It
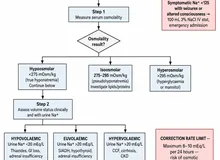
Serum osmolality reflects the total solute concentration in plasma and is tightly regulated at 275–295 mOsm/kg. The two major measured osmoles are sodium (and its paired anions, which contribute ~2 × Na) and glucose and urea (each contributing a small fraction). The standard formula captures all three. Any additional substance dissolved in plasma — ethanol, methanol, ethylene glycol, mannitol, glycerol — will raise the measured osmolality without appearing in the calculated value, creating an osmolal gap.
An osmolal gap > 10 mOsm/kg in the appropriate clinical context (unexplained AMS, high anion gap, history of ingestion) should trigger an emergency toxic alcohol screen and empirical antidotal therapy (fomepizole for methanol and ethylene glycol; ethanol infusion where fomepizole is unavailable). Early recognition is critical because the parent compounds are far less toxic than their metabolites — formic acid (from methanol) causes blindness and death, while glycolic and oxalic acid (from ethylene glycol) cause severe AKI and oxalate crystalluria.
Serum Osmolality & Osmolal Gap Calculator
Enter serum sodium, glucose, and BUN/urea. Adding the lab-measured osmolality enables computation of the osmolal gap. Results update automatically on input.
⚕ The osmolal gap is a screening test only. A normal gap does not exclude toxic alcohol ingestion in the early phase. Always correlate with clinical context and send a toxic alcohol screen when ingestion is plausible.
Next Steps
Use the result to support — not replace — clinical judgment.
- Interpret the value against the targets shown in the calculator and the Evidence section below, in the context of the full clinical picture.
- Trend serial measurements rather than acting on a single result; confirm abnormal or unexpected values before changing management.
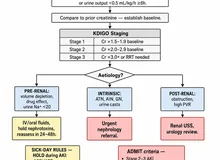
- Apply the relevant KDIGO / specialty-guideline threshold and document the indication.
- Escalate or refer to nephrology when results are out of range, rapidly changing, or discordant with the clinical picture — and discuss the implications with the patient.
Evidence & References
Formula & Equations
| Quantity | Equation |
|---|---|
| Calculated serum osmolality (mOsm/kg) | 2 × Na⁺ (mEq/L) + Glucose (mg/dL) / 18 + BUN (mg/dL) / 2.8 |
| Osmolal gap (mOsm/kg) | Measured osmolality − Calculated osmolality |
Unit conversion factors used internally
| Lab value | Conversion |
|---|---|
| Glucose mmol/L → mg/dL | multiply by 18 |
| Urea mmol/L → BUN mg/dL | multiply by 2.8 |
Osmolal gap interpretation
| Osmolal gap | Interpretation | Differential |
|---|---|---|
| Normal (< 10) | No significant unmeasured osmoles | Does not fully exclude early toxic alcohol ingestion |
| Elevated (≥ 10) | Unmeasured osmole present | Methanol · Ethylene glycol · Isopropyl/ethyl alcohol · Mannitol · Glycerol · Pseudohyponatremia (lipid, protein) |
The normal calculated osmolality range is 275–295 mOsm/kg. Values outside this range without a clear explanation (hyperglycemia, azotemia) warrant further evaluation. Note that ethanol, if present, is not measured separately in the standard formula — its contribution must be subtracted: gap corrected for ethanol = measured osm − calculated osm − (ethanol mg/dL / 4.6).
Evidence & References
The standard osmolality formula (2 × Na + glucose/18 + BUN/2.8) and the concept of the osmolal gap were systematically described by Smithline and Gardner in 1976 as a clinical tool to detect unmeasured osmoles. The threshold of 10 mOsm/kg is derived from normal reference ranges observed in healthy individuals and is widely used in clinical practice, though the reference range varies slightly across laboratories (some use < 6, others < 12).
- Smithline N, Gardner KD Jr. Gaps — anionic and osmolal. JAMA. 1976;236(14):1594–1597.
- Kruse JA, Cadnapaphornchai P. The serum osmole gap. J Crit Care. 1994;9(3):185–197.
- Purssell RA, Pudek M, Brubacher J, Abu-Laban RB. Derivation and validation of a formula to calculate the contribution of ethanol to the osmolal gap. Ann Emerg Med. 2001;38(6):653–659.