- Enter your systolic BP (upper number) and diastolic BP (lower number) in mmHg. Use the average of 2–3 readings taken while seated and rested for at least 5 minutes.
- Select your CKD or clinical profile — this determines the evidence-based BP target that applies to you.
- Select the number of BP medications you are currently taking — this shapes the therapeutic recommendation.
- Results update automatically: MAP, pulse pressure, your profile-specific BP target, and a plain-language assessment with recommended next steps.
- For home monitoring: measure every morning before medications and before breakfast, in the same arm, for at least 5–7 days. Bring your log to every clinic appointment.
All computation runs in your browser; no values are stored or transmitted.
When to Use
Use this tool when reviewing a blood pressure reading in any patient with CKD, diabetes, hypertension, or post-kidney transplant status. It computes mean arterial pressure (MAP) and pulse pressure from a single BP pair, then maps the result to the correct KDIGO 2024 target for the patient's clinical profile.
Appropriate population
Adults with any of the following: CKD (any stage, with or without proteinuria), CKD plus diabetes mellitus, maintenance dialysis (hemodialysis or peritoneal dialysis), post-kidney transplant, or essential hypertension without CKD. Use the average of two or more resting office readings, or a home BP average taken over 5–7 mornings before medications for greatest accuracy.
When NOT to rely on it alone
A single BP reading is insufficient for treatment decisions — BP is inherently variable. Do not use this calculator to start or stop antihypertensive therapy without physician evaluation. White-coat hypertension (elevated in clinic, normal at home) and masked hypertension (normal in clinic, elevated at home) are common in CKD and require 24-hour ambulatory BP monitoring for confirmation. If the result shows hypertensive crisis (SBP ≥180 or DBP ≥120), seek immediate medical attention.
Pearls & Pitfalls
Home BP is more reliable than office BP in CKD
White-coat effect inflates office readings by 10–15 mmHg in up to 30% of CKD patients. KDIGO 2021 prioritizes standardized office BP (average of two readings on two separate visits) and recommends home BP monitoring to guide treatment. A systolic home BP average >135 mmHg is the home-equivalent of office >140 mmHg.
Sodium restriction amplifies every antihypertensive drug
Dietary sodium >2 g/day blunts the effect of ACE inhibitors, ARBs, and even diuretics. In CKD, sodium restriction is not optional — it is pharmacological. Every 1 g/day reduction in sodium intake lowers BP by approximately 3–5 mmHg systolic and reduces proteinuria independently.
Wide pulse pressure in CKD: do not ignore it
Pulse pressure >60 mmHg signals vascular stiffness and calcification — common in dialysis patients and those with long-standing CKD. Even with controlled mean BP, a high pulse pressure is an independent predictor of cardiovascular events. Correcting mineral metabolism (phosphorus, PTH, vitamin D) is the only modifiable driver of vascular calcification in CKD.
First-line agents for CKD with proteinuria
ACE inhibitors and ARBs are the preferred agents when UACR ≥30 mg/g — they lower intraglomerular pressure beyond their systemic BP effect, reducing proteinuria by 30–50%. Do not combine an ACE inhibitor with an ARB (dual RAAS blockade increases AKI and hyperkalemia risk without additional benefit, per ONTARGET). Monitor serum creatinine and potassium 1–2 weeks after starting or dose-escalating a RAAS blocker.
Why Use It
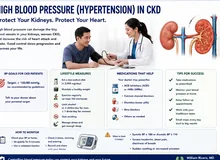
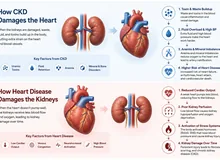
Hypertension accelerates CKD progression through two mechanisms: systemic hypertension damages the glomerular capillaries directly, and high intraglomerular pressure (worsened by a high MAP) drives proteinuria and podocyte injury independent of systemic BP. For every 10 mmHg reduction in systolic BP, the rate of GFR decline slows by approximately 30% in proteinuric CKD. The pulse pressure — the arithmetic difference between systolic and diastolic — reflects arterial stiffness; a wide pulse pressure (>60 mmHg) in CKD signals vascular calcification driven by disordered calcium-phosphorus metabolism and predicts cardiovascular mortality independently of mean BP. Knowing both MAP and pulse pressure from a single reading allows a more complete cardiovascular risk assessment than systolic BP alone.
Blood Pressure Calculator — MAP, Pulse Pressure & CKD Target Checker
Enter your blood pressure reading and clinical profile to calculate MAP and pulse pressure, and see whether your BP meets the KDIGO 2024 target for your specific CKD and proteinuria status.
⚕ MAP = DBP + (SBP − DBP) ÷ 3. Pulse pressure = SBP − DBP; PP >60 mmHg suggests arterial stiffness, common in CKD and associated with increased cardiovascular risk. BP targets per KDIGO 2024 and 2021 CKD BP Guideline. Home BP monitoring (morning before medications) is more reliable than office readings for CKD patients. This tool is educational — antihypertensive adjustments require physician evaluation.
Next Steps
Use the result to support — not replace — clinical judgment.
- Interpret the value against the targets shown in the calculator and the Evidence section below, in the context of the full clinical picture.
- Trend serial measurements rather than acting on a single result; confirm abnormal or unexpected values before changing management.
- Apply the relevant KDIGO / specialty-guideline threshold and document the indication.
- Escalate or refer to nephrology when results are out of range, rapidly changing, or discordant with the clinical picture — and discuss the implications with the patient.
Evidence & References
Formula & Equations
| Quantity | Equation |
|---|---|
| Mean Arterial Pressure (MAP) | DBP + (SBP − DBP) ÷ 3 [equivalently: (SBP + 2×DBP) ÷ 3] |
| Pulse Pressure (PP) | SBP − DBP (mmHg) |
KDIGO 2024 BP Target Reference
| Clinical Profile | Target | Rationale |
|---|---|---|
| CKD with proteinuria (UACR ≥30 mg/g) | <130/80 mmHg | Tighter control reduces intraglomerular pressure and proteinuria-driven progression |
| CKD with diabetes mellitus | <130/80 mmHg | Dual benefit: kidney protection and cardiovascular risk reduction |
| CKD without proteinuria (UACR <30 mg/g) | <140/90 mmHg | Standard target; if UACR rises ≥30, tighten to <130/80 |
| On dialysis (HD or PD) | <140/90 mmHg (pre-dialysis) | Optimal dry weight via ultrafiltration is the primary BP intervention before adding agents |
| Post kidney transplant | <130/80 mmHg | Calcineurin inhibitors cause vasoconstriction; CCBs first-line |
| Hypertension without CKD | <140/90 mmHg | Standard ACC/AHA / ESH 2023 target |
MAP target: generally <100 mmHg; MAP 70–100 mmHg ensures adequate organ perfusion while limiting glomerular hypertension. The MAP formula shown uses the standard clinical approximation; the exact formula integrates the arterial waveform but gives numerically similar results at normal heart rates.
Evidence & References
The BP targets in this calculator follow two landmark guidelines. The KDIGO 2021 Guideline for the Management of Blood Pressure in CKD, which synthesized over 130 randomized trials, provided the first CKD-specific framework distinguishing proteinuric from non-proteinuric patients and explicitly set a <120 mmHg systolic target for eligible individuals following SPRINT data. The 2017 ACC/AHA Hypertension Guideline established the general framework and the universal <130/80 mmHg goal for patients with CKD, diabetes, or established cardiovascular disease.
- KDIGO 2021 Clinical Practice Guideline for the Management of Blood Pressure in Chronic Kidney Disease. Kidney International. 2021;99(3S):S1–S87.
- Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults. Hypertension. 2018;71(6):e13–e115.