Why Machine Assignment Matters
In the Philippines, hemodialysis centers operate up to 3–4 sessions per machine per day. Each machine’s extracorporeal circuit, ports, and surfaces can harbor bloodborne viruses if infection control protocols are breached. PSN 2024 and DOH AO 2012-0001 mandate strict machine separation by serostatus — not as a bureaucratic requirement, but because nosocomial HBV and HCV transmission in dialysis units is a documented, preventable harm.
Hepatitis B Virus (HBV)
Extremely environmentally stable — survives on dry surfaces for more than 7 days. Standard cleaning without dedicated machine separation is insufficient to prevent transmission. High viral loads in HBsAg-positive patients amplify risk.
Hepatitis C Virus (HCV)
Spreads through shared machines, contaminated dialysis ports, blood-contaminated hands, and inadequate glove changes between patients. Machine separation is mandatory even after successful antiviral treatment in most Philippine HD centers.
HIV
Lower environmental stability than HBV/HCV and inactivated by standard disinfection. Nevertheless, a designated machine is required per Philippine center policy and RA 11166 protections. Universal precautions apply to every session for every patient.
The Window Period: The Most Dangerous Gap
A patient can be HBsAg-negative yet fully infectious during the first 1–8 weeks after HBV exposure. During this window, only Anti-HBc IgM is positive. Relying on HBsAg alone misses these cases entirely. Anti-HBc IgM testing is mandatory for all new patients.
The four machine categories — Non-Isolation, Unknown/New, HBV-Isolation, and HCV-Isolation — are described in detail in Section 2. HIV assignment is covered in Section 7.
The Four Standard Machine Categories
Philippine HD centers are required by DOH AO 2012-0001 to maintain at minimum the following dedicated machine types. Each category is mutually exclusive — a machine assigned to one group must not be used by patients from another group without completing enhanced inter-session disinfection as defined by center policy.
▮ Non-Isolation Machine
Who uses it: Patients with all serology negative (HBsAg−, Anti-HCV−, HIV−). Anti-HBs ≥10 mIU/mL preferred (or documented vaccination series). Rules: Re-screen every 3 months. If any result becomes reactive, transfer immediately to the appropriate isolation machine.
▮ Unknown / New Patient Machine
Who uses it: Any patient with incomplete or pending serology (at least one of HBsAg, Anti-HCV, or HIV result is unavailable). Rules: Temporary assignment only. Treat as potentially infectious. Reassign within 1–2 sessions once all results are available. Do not use for known-seropositive patients.
▮ HBV-Isolation Machine
Who uses it: HBsAg-positive patients AND window-period patients (Anti-HBc IgM positive, regardless of HBsAg result). Rules: Dedicated machine AND dedicated nursing staff per session. Never shared with HCV-only or HIV-only patients. HBV + HIV co-infected patients use this machine with additional HIV precautions.
▮ HCV-Isolation Machine
Who uses it: Anti-HCV reactive patients (confirmed or pending confirmation). Rules: Separate from HBV-isolation machines. In most Philippine HD centers, machine assignment persists for life once Anti-HCV is reactive, regardless of HCV RNA status. HCV + HIV co-infected patients use this machine with additional HIV precautions.
Isolated Anti-HBc: A Special Case
Pattern: HBsAg−, Anti-HBs− or low, Anti-HBc Total +, Anti-HBc IgM−. This may represent old resolved HBV infection with waned Anti-HBs, occult HBV, or a false positive. Obtain HBV DNA and consult the nephrologist. Assignment to non-isolation is generally acceptable if HBV DNA is undetectable, but must not be assumed without physician review.
Never Use the HBV Machine for Non-HBV Patients
The HBV-isolation machine must never be used even temporarily for a seronegative patient. HBV contamination of the dialysate circuit, ports, and surfaces is extremely difficult to eliminate without a full enhanced disinfection cycle. One breach can cause seroconversion.

A chart of the four hemodialysis machine categories — Non-Isolation, Unknown or New, HBV-Isolation, and HCV-Isolation — showing who is assigned to each machine and the key safety rule for each.
Required Laboratory Tests Before Machine Assignment
Per PSN HD Guidelines 3rd Edition 2024, the following tests are mandatory before assigning any new patient to a hemodialysis machine. Incomplete results default to the Unknown/New Patient machine.
HBsAg — Hepatitis B Surface Antigen
The primary HBV screening test. If reactive → HBV-isolation machine immediately. A negative result does not rule out window period — proceed to Anti-HBc IgM.
Anti-HBs — Hepatitis B Surface Antibody (titer)
≥10 mIU/mL indicates protective immunity (vaccination or natural clearance). Guides booster decisions. A protective titer allows non-isolation assignment when all other serology is negative.
Anti-HBc Total (IgG + IgM combined)
Detects any prior HBV exposure. Must always be interpreted together with Anti-HBc IgM — cannot distinguish acute from chronic or resolved infection on its own.
Anti-HBc IgM — CRITICAL
Positive + HBsAg negative = HBV window period = patient is currently infectious → HBV-isolation machine immediately. This is the single most important test for window period detection. Never omit in new patients.
HBeAg and Anti-HBe
Hepatitis B e-antigen and antibody indicate viral replication phase and relative infectivity. These affect treatment decisions but do not change machine assignment — HBsAg-positive patients use the HBV machine regardless of HBeAg status.
HBV DNA (Quantitative PCR)
Required for: isolated Anti-HBc cases, pre-antiviral therapy baseline, HBsAg clearance evaluation, and treatment monitoring. Not required for initial machine assignment in most cases.
Anti-HCV — Hepatitis C Antibody
If reactive → assign to HCV-isolation machine pending confirmatory testing. Order HCV RNA PCR to confirm active viremia. Anti-HCV persists for life even after successful treatment.
HCV RNA PCR — Confirmatory / Quantitative
Detectable within 1–2 weeks of HCV infection — before Anti-HCV becomes reactive. Required to confirm active viremia after reactive Anti-HCV and for treatment monitoring (SVR12).
HIV 1/2 Ag/Ab Combo (4th generation)
If reactive → confirmatory Western Blot or supplemental antibody testing. See Section 7 for machine assignment. 4th-gen assays shorten the detection window to ~18 days by detecting both p24 antigen and IgM/IgG simultaneously.
CBC, ALT, AST, Creatinine — Baseline Panel
ALT/AST rising unexpectedly in a seronegative patient may precede serological positivity by 2–6 weeks. Unexplained ALT >2× ULN → re-test with Anti-HBc IgM and HBsAg immediately.
HBV Full Serology Interpretation Table
| HBsAg | Anti-HBs | Anti-HBc Total | Anti-HBc IgM | Interpretation | Machine Assignment |
|---|---|---|---|---|---|
| − | − | − | − | Susceptible; no prior HBV exposure | Non-Isolation after vaccination series |
| − | + (≥10) | − | − | Vaccine-induced immunity | Non-Isolation |
| − | + | + | − | Past infection; naturally immune | Non-Isolation |
| + | − | + | − | Chronic HBV carrier | HBV-Isolation |
| + | − | + | + | Acute HBV infection | HBV-Isolation |
| − | − | + | + | WINDOW PERIOD — patient IS infectious | HBV-Isolation ← CRITICAL |
| − | − | + | − | Isolated Anti-HBc (old exposure or false positive) | Physician Review Required — check HBV DNA |
| − | <10 | − | − | Vaccine non-responder or susceptible | Non-Isolation — re-vaccinate with high-dose series |

A step-by-step flowchart for reading hepatitis B blood tests, tracing the results down to the correct machine assignment and flagging the infectious window period when standard tests can still be negative.
Machine Allocation Decision Tool
Enter the patient’s serology results to receive an immediate machine assignment recommendation based on PSN 2024 guidelines. This tool is an educational aid — always confirm with the supervising nephrologist.
Machine Allocation Decision Tool
Enter the patient's serology results to receive a machine assignment recommendation based on PSN HD Guidelines (3rd Ed. 2024) and DOH AO 2012-0001.
Periodic Screening Schedule (PSN 2024)
All patients on maintenance hemodialysis require regular viral serology surveillance. Frequency increases when exposure is suspected or a new seropositive case is identified in the unit.
| Test | Baseline | Routine Interval | Accelerated Interval | Notes |
|---|---|---|---|---|
| HBsAg | Required | Every 3 months | Monthly if exposure suspected | All non-immune patients |
| Anti-HBs titer | Required | Every 6 months | After booster doses | Booster if <10 mIU/mL |
| Anti-HBc IgM | Required (new patients) | Not routine — order if seroconversion suspected | Immediately if ALT rises or HBsAg converts | Window period detection |
| Anti-HCV | Required | Every 3 months | Monthly during center outbreak | Confirm reactive with HCV RNA PCR |
| HIV Ag/Ab combo | Required | Every 6–12 months | After needlestick or high-risk exposure | 4th-gen assay preferred |
| HBV DNA | When clinically indicated | When indicated | — | Isolated Anti-HBc, pre-treatment, HBsAg clearance |
| HCV RNA (PCR) | After reactive Anti-HCV | Treatment monitoring | — | SVR confirmation at 12 weeks post-treatment |
| ALT / AST | Required | Monthly | — | Rising ALT may precede seroconversion by weeks |
Rising ALT: Act Before Seroconversion
An unexplained rise in ALT (>2× ULN) in a seronegative dialysis patient should prompt immediate re-testing with Anti-HBc IgM and HBsAg — even if the previous test was negative less than a month ago. ALT elevation commonly precedes serological positivity by 2–6 weeks. Early detection allows earlier machine reassignment and contact tracing.
Cluster Response Screening
If a new HBV or HCV seroconversion is identified, DOH AO 2012-0001 requires screening of all patients who shared the same machine within the preceding 3–6 months. Do not wait for the next routine screening cycle.
Hepatitis B Vaccination Protocol for Dialysis Patients
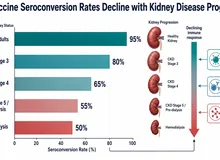
CKD and dialysis patients have impaired immune responses due to uremia-related immunosuppression. Seroconversion rates after standard HBV vaccination are significantly lower than in the general population. Higher-dose schedules are required.
Standard Pre-Dialysis / CKD Schedule
Engerix-B 20 mcg (1 mL) IM at months 0, 1, 6
— or —
Recombivax HB 10 mcg IM at months 0, 1, 6
Check Anti-HBs titer 1–2 months after final dose.
Target: Anti-HBs ≥10 mIU/mL
High-Dose Dialysis Schedule (Preferred)
Engerix-B 40 mcg (2×1 mL) IM at months 0, 1, 2, 6
— or —
Recombivax HB 40 mcg (dialysis formulation) at months 0, 1, 6
Check Anti-HBs titer 4–8 weeks after final dose.
Annual titer check; booster if <10 mIU/mL
Machine Assignment Based on Vaccination and Titer Status
- Anti-HBs ≥10 mIU/mL + all other serology negative → Non-isolation machine
- Anti-HBs <10 mIU/mL + all other serology negative → Non-isolation machine; initiate or restart high-dose vaccination series; re-check titer in 2 months
- Non-responder (Anti-HBs <10 mIU/mL after two complete high-dose series) → Non-isolation machine; consider HBIG for post-exposure prophylaxis; apply enhanced precautions; document non-responder status
- HBsAg pending → Unknown/New machine until result confirmed
Non-Responders (approximately 5–10% of dialysis patients)
After two complete high-dose series, approximately 5–10% of dialysis patients remain Anti-HBs <10 mIU/mL. These patients are permanently susceptible to HBV. If exposed, they should receive HBIG (0.06 mL/kg IM) as soon as possible (within 24 hours preferred). Document non-responder status prominently in the chart.
HIV and Machine Assignment
Legal Right to Dialysis
HIV is not a barrier to hemodialysis. Republic Act No. 11166 (Philippine HIV and AIDS Policy Act, 2018) prohibits any health facility from denying life-sustaining treatment based solely on HIV status. Denial of dialysis to a person living with HIV is a violation of Philippine law.
Per PSN HD Guidelines 2024 and DOH policy, HIV-positive patients are assigned to a machine separate from the non-isolation pool. Philippine HD center practice varies: some maintain a dedicated HIV machine; others use the HCV-isolation machine with enhanced between-session disinfection (1:10 sodium hypochlorite cycle). Both approaches are acceptable provided universal precautions are strictly applied.
Unlike HBV and HCV, HIV has low environmental stability and is inactivated by standard dialysis machine disinfection procedures. The transmission risk through the dialysis machine circuit is extremely low with proper precautions — far lower than through needlestick or blood splash.
Confidentiality (RA 11166): A patient’s HIV status must not be disclosed without informed consent. Machine labels must not publicly identify a patient as HIV-positive. Use internal coded labels (e.g., machine number with session codes) consistent with center infection control policy.
HIV Alone (no HBV/HCV co-infection)
Use the center’s HIV-designated machine, or the HCV machine with enhanced between-session disinfection. Apply HIV universal precautions (PPE: gown + gloves + eye protection every session). Never co-assign with HBsAg-positive patients on the same machine.
HIV + HBV Co-infection (HBsAg+)
HBV-isolation machine ALWAYS takes precedence. Apply HIV universal precautions in addition to standard HBV protocols. The HBV machine must not be shared with HCV-negative patients or HIV-only patients without enhanced disinfection.
HIV + HCV Co-infection (Anti-HCV+)
Use the HCV-isolation machine. Apply both HIV and HCV precautions simultaneously. Do not share the machine with HCV-negative HIV-positive patients without enhanced disinfection per center policy.
HIV + HBV Co-infection: HBV Protocol Takes Priority
When a patient is both HIV-positive and HBsAg-positive, the HBV-isolation machine is used — full stop. Do not assign to an HIV or HCV machine. Add HIV universal precautions on top of standard HBV protocols.
When a Patient Seroconverts
Seroconversion — a previously seronegative patient testing newly positive for HBsAg or Anti-HCV — is a serious unit event requiring immediate, coordinated action. Every seroconversion should be treated as a potential failure of infection control protocols until proven otherwise.
Same-Day Actions Required
- Notify supervising nephrologist immediately (within the same day)
- Transfer patient to the appropriate isolation machine for ALL future sessions
- If seroconversion is discovered mid-session: complete the session with strict contact precautions, then perform enhanced machine disinfection before any subsequent use
- Complete a seroconversion Incident Report
- Notify HD Unit Supervisor and Infection Control Officer
- Review machine usage log and identify all patients on the same machine for the past 3–6 months
Document
Record: date of last negative test, date of first positive result, machine number, session shift, nursing staff assigned. Preserve all disinfection logs.
Notify and Report
Nephrologist within 24 hours; HD Medical Director within 48 hours. If cluster (≥2 new seroconversions within 90 days on same shift or machine): mandatory DOH notification within 24 hours per AO 2012-0001.
Reassign Machine
All future sessions: HBV-isolation (HBsAg+) or HCV-isolation (Anti-HCV+). Complete enhanced machine disinfection of implicated machine and document.
Contact Tracing
Review machine usage logs. Identify all patients who dialyzed on the same machine in the preceding 3–6 months. Build a contact tracing list.
Re-screen Contacts
For HBV exposure: HBsAg + Anti-HBc IgM within 2–4 weeks; repeat at 8 and 16 weeks.
For HCV exposure: Anti-HCV + HCV RNA within 2–4 weeks; repeat at 8 and 16 weeks.
Post-Exposure Prophylaxis (HBV)
Unvaccinated patients or those with Anti-HBs <10 mIU/mL exposed to HBV: HBIG 0.06 mL/kg IM plus first HBV vaccine dose as soon as possible (within 24 hours preferred, up to 7 days).
Investigate Source
Review staff universal precautions practices, glove change compliance, machine disinfection logs, water system records. Identify the most likely transmission event. Document findings.
Staff Re-training and Final Report
Conduct a staff re-training session on universal precautions and machine protocols. Document attendance. Submit final incident report to DOH if classified as a cluster. File all records for DOH inspection.

A timeline showing what a dialysis unit should do after a new infection is detected, from immediate actions on Day 0 through notifications, investigation, and re-screening contacts over the following weeks.
Interactive Seroconversion Protocol Checklist
Use the tool below to generate and track a step-by-step seroconversion protocol checklist for your unit.
Seroconversion Protocol Checklist
For use when a patient on the HD unit tests newly positive for HBV or HCV. Select the type of seroconversion and the date of discovery to generate a step-by-step actionable checklist.
Superimposed Contagious Infections
Dialysis patients may develop additional transmissible infections (active TB, influenza, COVID-19, MRSA) on top of their existing hepatitis or HIV status. These dual situations require two simultaneous, independent decisions.
Two Independent Decisions
Decision 1 — Which machine? Determined by hepatitis/HIV serology. This does not change based on superimposed infections.
Decision 2 — Where and when in the HD unit? Determined by the superimposed contagious infection (airborne, droplet, or contact precautions, shift timing, room placement).

A decision matrix showing that two separate choices guide care for a patient with an added infection: which machine to use (set by blood serology) and where and when to dialyze them (set by the type of precaution the new infection needs).
Active Pulmonary TB (PTB) in Dialysis Patients
Active PTB is Airborne
A patient with sputum AFB smear-positive, GeneXpert MTB/RIF-positive, or culture-positive pulmonary TB cannot dialyze in the open main HD room. This is an airborne-precautions infection. Appropriate location and timing arrangements must be made regardless of machine type.
| PTB Status | Machine (based on serology) | Location / Shift | Staff Precautions |
|---|---|---|---|
| Suspected PTB (workup pending) | Per HBsAg/HCV/HIV serology | Isolated room or last shift with doors open and windows maximally open | Fit-tested N95 respirator for all staff entering; surgical mask for patient |
| Confirmed PTB AFB smear-positive | Per HBsAg/HCV/HIV serology | Isolated room with airborne precautions (negative pressure if available); if unavailable, last shift in dedicated separate well-ventilated room | N95 for all entering staff; HEPA exhaust filter if available; minimize patient movement; patient wears surgical mask |
| PTB on DOTS ≥2 weeks + 3× AFB smear negative | Per HBsAg/HCV/HIV serology | May return to main HD room; no special location restriction | Standard precautions; continue TB medications |
| Latent TB (IGRA/TST+ only, no active disease) | Per HBsAg/HCV/HIV serology | Standard HD room; no isolation needed | Standard precautions; LTBI treatment if indicated |
DOH AO 2008-0003 mandates TB infection control in all health facilities, including HD centers. The Philippine NTP requires a minimum of 2 weeks of effective multi-drug therapy AND three consecutive negative AFB sputum smears before removing airborne precautions.
Other Transmissible Infections
| Infection | Transmission Route | Location / Shift | Machine Assignment |
|---|---|---|---|
| Active pulmonary TB | Airborne (droplet nuclei) | Isolated room or last shift + strong ventilation | Per HBV/HCV/HIV serology |
| Measles, Varicella (active) | Airborne | Isolated room; defer dialysis if hemodynamically stable and non-urgent | Per HBV/HCV/HIV serology |
| Influenza (confirmed) | Droplet | Consider last shift; separate from immunocompromised patients | Per HBV/HCV/HIV serology |
| COVID-19 (active) | Droplet + Airborne | Isolated room or designated COVID area; defer if non-urgent | Per HBV/HCV/HIV serology |
| MRSA / Skin infections | Contact | Contact precautions (gown + gloves); standard shift scheduling | Per HBV/HCV/HIV serology |
| C. difficile diarrhea | Contact (spores) | Contact precautions; consider last shift; sporicidal disinfection of surfaces | Per HBV/HCV/HIV serology |
| Scabies (confirmed) | Contact | Last shift; treat all close contacts before returning to normal schedule | Per HBV/HCV/HIV serology |
HBV/HCV Isolation + Active TB: The Most Complex Scenario
A patient requiring both HBV-isolation (or HCV-isolation) AND airborne precautions for active TB must dialyze in an isolated room on their designated isolation machine. This requires specific scheduling arrangements — the isolation machine must be physically moved to or reserved for the isolated room, or the patient must use the last shift with the isolation machine positioned in the well-ventilated area. Coordinate with the HD Medical Director and Infection Control Officer.
Co-infection Protocol Quick Reference Tool
Select the patient’s baseline serostatus and any active superimposed infection to receive combined protocol recommendations.
Co-infection Protocol Quick Reference
Select the patient’s baseline HD serology status and any superimposed active infection to receive the combined machine, location, PPE, and precaution recommendations.
Understanding IgM vs IgG: What Each Marker Means
IgM antibodies emerge early in primary infection (acute phase) and typically fade within 6–12 months. IgG antibodies develop later and persist for life. Confusing these two immunoglobulin classes is a recognized cause of incorrect machine assignment, particularly in missing the HBV window period.
Hepatitis B — IgM vs IgG
| Marker | Timing | What It Means | Machine Implication |
|---|---|---|---|
| Anti-HBc IgM | Appears 1–2 weeks after exposure; peaks 3–6 weeks; fades by 6–12 months | ACUTE infection OR window period. Patient is infectious even if HBsAg is negative. | HBV-Isolation Machine — IMMEDIATELY |
| Anti-HBc IgG | Develops after IgM; persists for life | Past exposure (resolved or chronic HBV). Must be combined with HBsAg to interpret. | Interpret with full profile; see serology table in Section 3 |
| Anti-HBc Total | Detects both IgM and IgG | Indicates any prior exposure. Cannot alone distinguish acute from chronic from resolved. | Always order IgM to complete interpretation |
| Anti-HBs | Appears during recovery or after vaccination | Protective immunity. ≥10 mIU/mL = protected. | ≥10 mIU/mL + negative serology → Non-isolation |
| HBeAg | During active viral replication | High infectivity; guides treatment decisions | Does not change machine assignment independently |
THE WINDOW PERIOD: HBsAg NEGATIVE + Anti-HBc IgM POSITIVE
This is the single most important serological interpretation in HD infection control. The patient IS infectious. HBsAg disappears 1–6 weeks before Anti-HBs appears. During this gap, only Anti-HBc IgM is positive. Any clinician or nurse who relies on HBsAg alone will miss this entirely. Always assign to the HBV-isolation machine.
HBV Window Period Timeline
| Phase | Weeks Post-Exposure | HBsAg | Anti-HBc IgM | Anti-HBs | Machine |
|---|---|---|---|---|---|
| Pre-infection | 0 | − | − | ± | Non-Iso |
| Early acute / Window | 1–8 | − | + | − | HBV-Iso |
| Established acute | 4–16 | + | + | − | HBV-Iso |
| Resolution / Clearance | 12–24 | − | Fading | + | Non-Iso (confirm) |
| Chronic carrier | >24 | + | − | − | HBV-Iso |
Hepatitis C — Why There Is No IgM Test
Anti-HCV is an IgG antibody. Unlike HBV, there is no validated Anti-HCV IgM test for routine clinical use in dialysis settings. A reactive Anti-HCV persists for life — even after spontaneous clearance or successful antiviral treatment. Reactivity does not mean the patient is currently infectious.
To determine current HCV infectivity, HCV RNA PCR is required. HCV RNA becomes detectable within 1–2 weeks of infection — weeks before Anti-HCV becomes reactive. HCV RNA is the definitive test for active viremia.
Cleared HCV: Can the Patient Move to Non-Isolation?
Anti-HCV+ but undetectable HCV RNA at 12 weeks post-treatment (SVR12): some international guidelines permit reassignment to non-isolation. In the Philippines, most HD centers maintain HCV-machine assignment permanently once Anti-HCV is reactive, to simplify operations and minimize risk in resource-limited settings. Consult the HD Medical Director and current PSN 2024 guidance before any reassignment.
HIV — 4th Generation Testing and the Window Period
HIV 4th-generation Ag/Ab combo tests detect both p24 antigen and IgM/IgG antibodies simultaneously. This shortens the detection window period to approximately 18 days (vs. 22 days for 3rd-generation IgG-only assays). Any reactive HIV combo test must be confirmed with Western Blot or supplemental antibody testing before final machine assignment and treatment decisions.
Philippine Regulatory Summary
The following documents constitute the legal and clinical basis for machine assignment decisions in Philippine HD centers. Compliance is not optional — non-compliance with DOH standards affects PhilHealth accreditation and exposes the facility to administrative and legal liability.
| Document | Issuing Body | Year | Key Machine-Assignment Requirement |
|---|---|---|---|
| PSN Hemodialysis Standards and Clinical Practice Guidelines, 3rd Edition | Philippine Society of Nephrology | 2024 | Mandatory HBV/HCV machine isolation; screening schedule; vaccination protocol; seroconversion response requirements |
| Administrative Order No. 2012-0001 | Department of Health | 2012 | Licensing standards for dialysis facilities; dedicated isolation machines required; cluster outbreak mandatory reporting within 24 hours |
| Administrative Order No. 2008-0003 | Department of Health | 2008 | TB infection control in all health facilities; mandatory application to HD centers; includes ventilation requirements and PPE standards |
| PhilHealth Circular No. PC 2024-0023 | Philippine Health Insurance Corp. (PhilHealth) | 2024 | ₱6,350/session; 156 covered sessions/year; facility must comply with DOH AO 2012-0001 standards to maintain accreditation |
| Republic Act No. 11166 | Congress of the Philippines | 2018 | HIV and AIDS Policy Act: non-discrimination; mandatory confidentiality; prohibition on denial of life-sustaining treatment based on HIV status |
| NTP Manual of Procedures, 5th Edition | DOH — National TB Program | 2014 | DOTS protocol; AFB clearance criteria (≥2 weeks effective treatment + 3× negative AFB smears) for removing airborne precautions |
PhilHealth Accreditation
PhilHealth accreditation for hemodialysis facilities requires full compliance with DOH AO 2012-0001, including proper machine separation. Failure to maintain isolation machines or to report cluster seroconversions can result in suspension or revocation of PhilHealth accreditation, with immediate financial impact on the facility and patients.
Cluster Outbreak Reporting
DOH AO 2012-0001 defines a cluster as ≥2 new seroconversions within the same HD unit within 90 days. Mandatory notification to the DOH is required within 24 hours of identification. Failure to report is an administrative violation. Prepare documentation: dates, patient identifiers (anonymized per privacy law), machines involved, and initial investigation findings.
Frequently Asked Clinical Questions
Can a patient with only isolated Anti-HBc (HBsAg−, Anti-HBs−, Anti-HBc IgG+, IgM−) use the non-isolation machine?
Usually yes, but only after physician review and with HBV DNA undetectable. Isolated Anti-HBc may represent: (1) old resolved HBV with waned Anti-HBs, (2) occult HBV infection with low-level viremia, or (3) false-positive reaction. Order HBV DNA quantitatively. If undetectable and Anti-HBc IgM is negative, non-isolation assignment is generally acceptable. Document the physician decision in the chart. Never assume non-isolation without this workup.
A patient’s Anti-HCV was reactive but HCV RNA PCR is undetectable — which machine?
In most Philippine HD centers: HCV-isolation machine, maintained permanently. Anti-HCV reactivity indicates past or current HCV infection. Even with undetectable HCV RNA (suggesting either spontaneous clearance or post-treatment SVR), the simplest and most cautious approach is permanent HCV-machine assignment. International guidelines allow reassignment after confirmed SVR12, but this requires HD Medical Director approval and adherence to current PSN 2024 guidance. When in doubt, maintain isolation.
A new patient arrives emergently for dialysis with no serology results yet. Which machine?
Unknown/New Patient machine. Treat as potentially infectious. Collect blood for the full viral serology panel immediately. Apply universal precautions. Reassign to the appropriate machine within 1–2 sessions once all results are available. Never assign to a non-isolation machine without completed serology.
Can HBV-positive and HCV-positive patients share the same isolation machine?
No. HBV-isolation and HCV-isolation machines must remain separate. A patient who is HBsAg+ uses the HBV-isolation machine exclusively; a patient who is Anti-HCV+ uses the HCV-isolation machine exclusively. Sharing between these two cohorts could result in super-infection (acquiring HCV if already HBsAg-positive, or HBV if already Anti-HCV-positive) and complicates clinical management significantly.
A patient on the HBV-isolation machine is found to have active PTB. What is the protocol?
Two simultaneous, independent protocols apply. (1) HBV-isolation machine: unchanged — this patient continues to use the HBV-isolation machine. (2) Airborne precautions: this patient cannot dialyze in the open main HD room. The HBV-isolation machine must be positioned in a separate isolated room or used in the final shift of the day with maximized ventilation. Staff wear N95 respirators. Coordinate machine placement with the HD Medical Director and Infection Control Officer.
How do I handle an HIV-positive patient who is also anti-HCV positive?
HCV-isolation machine, with additional HIV universal precautions applied throughout the session. HCV and HIV isolation are not additive in terms of machine requirements — the HCV-isolation machine is used. Staff must wear PPE appropriate for both HCV (universal precautions) and HIV (gown, gloves, eye protection) throughout the session. Do not use the same HCV-isolation machine for HIV-negative HCV-positive patients without enhanced disinfection between shifts, unless center policy explicitly addresses this.
We discovered a seroconversion two weeks ago but only just identified the affected machine. Is it too late to respond?
No — initiate the protocol immediately. The timeline for re-screening contact patients (within 2–4 weeks, then 8 and 16 weeks post-exposure) still applies from the estimated date of exposure. If that window has passed, accelerate re-screening immediately. Report the cluster to DOH as soon as it is identified, even if delayed. Document why the delay occurred as part of the incident report. Early vs. late detection does not affect the obligation to report and investigate.
Is a patient’s HIV status required to be disclosed on the machine label or the dialysis schedule?
No. Republic Act 11166 prohibits unauthorized disclosure of HIV status. Machine labels and schedule boards must use coded identifiers consistent with your center’s infection control policy. Only staff with a direct clinical need-to-know may be informed of a patient’s HIV status, and only within the constraints of RA 11166. Any public labeling that reveals HIV status is a violation of the law and subjects the facility to legal liability.
References and Guideline Sources
Philippine Guidelines and Regulations
- 1.Philippine Society of Nephrology. Hemodialysis Standards and Clinical Practice Guidelines, 3rd Edition. Manila: PSN; 2024. Available at: psn.org.ph PH
- 2.Department of Health Philippines. Administrative Order No. 2012-0001: Standards for Licensing and Operation of Dialysis Facilities. Manila: DOH; 2012. PH
- 3.Department of Health Philippines. Administrative Order No. 2008-0003: Guidelines for the Prevention and Control of Tuberculosis Transmission in Health Care Facilities. Manila: DOH; 2008. PH
- 4.Philippine Health Insurance Corporation. PhilHealth Circular No. PC 2024-0023: Updated Coverage for Hemodialysis and Related Renal Replacement Procedures. Manila: PhilHealth; 2024. PH
- 5.Republic of the Philippines. Republic Act No. 11166: An Act Strengthening the Comprehensive Policy on Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS). Manila: Congress of the Philippines; 2018. PH
- 6.Department of Health Philippines — National Tuberculosis Program. Manual of Procedures for the National Tuberculosis Control Program, 5th Edition. Manila: DOH-NTP; 2014. PH
International Guidelines and References
- 7.Kidney Disease: Improving Global Outcomes (KDIGO). KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. 2024;105(4S):S117–S314. INT
- 8.Centers for Disease Control and Prevention (CDC). Recommendations for Preventing Transmission of Infections Among Chronic Hemodialysis Patients. MMWR Recomm Rep. 2001;50(RR-5):1–43. [Historical reference; cited for background context only — not a Philippine regulatory mandate] INT
- 9.KDIGO. Clinical Practice Guidelines for the Prevention, Diagnosis, Evaluation, and Treatment of Hepatitis C in Chronic Kidney Disease. Kidney Int. 2008;73(Suppl 109):S1–S99. INT
- 10.Terrault NA, Lok ASF, McMahon BJ, et al. Update on Prevention, Diagnosis, and Treatment of Chronic Hepatitis B: AASLD 2018 Hepatitis B Guidance. Hepatology. 2018;67(4):1560–1599. INT
- 11.European Association for the Study of the Liver (EASL). EASL 2017 Clinical Practice Guidelines on the Management of Hepatitis B Virus Infection. J Hepatol. 2017;67(2):370–398. INT
- 12.Fabrizi F, Donato FM, Messa P. Association Between Hepatitis B Virus and Chronic Kidney Disease: A Systematic Review and Meta-Analysis. Ann Hepatol. 2017;16(1):21–47. INT
- 13.UK Renal Association / British HIV Association (BHIVA). Management of Blood-Borne Viruses in Adult Renal Units, 4th Edition. London; 2018. INT
- 14.World Health Organization. Guidelines for the Prevention, Care and Treatment of Persons with Chronic Hepatitis B Infection. Geneva: WHO; 2015. INT
- 15.World Health Organization. Guidelines for the Care and Treatment of Persons Diagnosed with Chronic Hepatitis C Virus Infection. Geneva: WHO; 2018. INT
- 16.World Health Organization. WHO Guidelines on Tuberculosis Infection Prevention and Control. Geneva: WHO; 2019 Update. INT
- 17.European Renal Association — European Dialysis and Transplant Association (ERA-EDTA). Recommendations for the Management of Hepatitis B and Hepatitis C in Patients on Chronic Hemodialysis. Nephrol Dial Transplant. 2010;25(3):671–678. INT
- 18.Fabrizi F, Messa P, Dixit V, Gish R, Martin P. Hepatitis C Virus Infection and Dialysis: A Systematic Review. ASAIO J. 2007;53(5):543–549. INT
- 19.Barril G, Bartolomé J. Hepatitis C and Dialysis: A New Perspective on a Complex Issue. NDT Plus. 2008;1(Suppl 1):i10–i14. INT
- 20.Kidney Health Australia (KHA-CARI). Caring for Australasians with Renal Impairment — Viral Hepatitis in Dialysis: Updated Guidelines. 2017. INT