- Select your stone type from the dropdown. If stone analysis was performed after passage or surgery, use that result. If unknown (e.g., first episode without stone capture), choose "Unknown / first stone" to receive general prevention guidance.
- Enter your body weight in kilograms. This is used to contextualise minimum fluid requirements alongside the urine output target.
- Enter your most recent eGFR (estimated glomerular filtration rate) in mL/min/1.73m². This is essential — patients with CKD G4 (eGFR <30) receive a fluid-restricted target and a note to discuss with their nephrologist before significantly increasing intake.
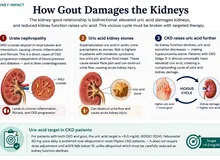
- Optionally enter your serum uric acid level if available. Elevated uric acid (above 6.0 mg/dL) triggers additional uricosuric guidance even in non-uric-acid stone types, since hyperuricosuria contributes to calcium oxalate stone formation.
All computation runs in your browser — no values are stored or transmitted. Print or screenshot the result to share with your nephrologist or urologist.
When to Use
Use this tool for any patient with a history of kidney stones (nephrolithiasis) or ureterolithiasis who needs a personalised daily fluid intake target and stone-type-specific dietary guidance. It is especially useful at first stone episode, at follow-up after stone passage or lithotripsy, and when serial urine output monitoring is being initiated.
Appropriate use
- Adults aged 18 and older with one or more episodes of kidney stone disease
- Patients with known stone composition (from stone analysis or imaging) or suspected stone type based on metabolic workup
- Patients with CKD who form stones — the calculator adjusts fluid targets for eGFR <30 and <45 mL/min/1.73m²
- Patients beginning a 24-hour urine stone risk assessment (provides context for urine output targets)
- Dietary counselling sessions: the output includes stone-type-specific Filipino-context food guidance
Limitations — when NOT to rely on it alone
- This calculator does not replace a formal 24-hour urine metabolic workup (oxalate, citrate, calcium, uric acid excretion), which is the gold standard for recurrent stone formers
- Do not dramatically increase fluid intake without first discussing with a nephrologist if eGFR is <30 mL/min/1.73m² — fluid overload risk is real in advanced CKD
- Struvite (infection) stones require surgical removal and antibiotic treatment — dietary measures and fluid intake alone are insufficient
- Cystine stones require specialist management; fluid targets here (3 L/day) are a floor, not a ceiling
Pearls & Pitfalls
The colour rule is the most practical daily guide
Patients who track their fluid intake numerically often find it burdensome and abandon the goal. Teach the urine colour rule instead: pale yellow to clear means adequate hydration; dark yellow or amber means more fluid is needed now. This single heuristic has been shown to improve adherence over long-term follow-up. Keep a glass of water by the bed — the morning urine void is the most concentrated of the day and the most likely to trigger crystal nucleation.
Do not restrict calcium — eat it with meals
For calcium oxalate stone formers (the majority), restricting dietary calcium is a common and harmful misconception. Dietary calcium binds oxalate in the gut, preventing its absorption and urinary excretion. Low calcium intake paradoxically increases urinary oxalate and stone risk. The correct advice is to maintain adequate calcium intake (500–1000 mg/day from food) taken with oxalate-containing foods. Calcium supplements taken between meals, however, do increase hypercalciuria and should be avoided.
Pitfalls to avoid
- Fluid restriction without nephrologist guidance in advanced CKD: eGFR <30 patients may develop fluid overload — always individualise.
- Treating struvite stones with diet alone: these require antibiotics and often surgical stone removal; dietary changes are adjunctive only.
- Assuming one stone type equals lifelong risk: new stone episodes can be a different type — always capture and analyse any passed stone.
- Vitamin C mega-dosing: Vitamin C (ascorbic acid) is metabolised to oxalate — doses above 200 mg/day significantly increase urinary oxalate in calcium oxalate stone formers.
- Not checking a 24-hour urine in recurrent formers: this calculator provides targets, but only a 24-hour urine stone risk panel identifies the specific metabolic defect driving recurrence.
Why Use It
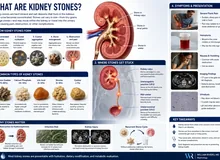
Kidney stones form when the concentration of stone-forming solutes (calcium, oxalate, uric acid, phosphate, cystine) in the urine exceeds the solubility threshold — a state called supersaturation. The single most effective intervention across all stone types is diluting the urine by increasing fluid intake to achieve a urine output of at least 2.5 litres per day. This reduces supersaturation, slows crystal nucleation, and significantly cuts recurrence rates.
In the Philippine climate, insensible losses (sweat, respiration) are higher than in temperate countries — typically 0.5 to 1.0 litres per day above the basal minimum. This means fluid intake targets must be set proportionally higher than the urine output target alone. A practical colour-based guide: urine should appear pale yellow to clear at all times; dark yellow or amber urine reliably signals under-hydration.
Beyond hydration volume, each stone type has distinct dietary risk factors. Calcium oxalate stones (the most common, comprising about 70% of cases) are driven by high dietary oxalate and low calcium intake — counterintuitively, restricting dietary calcium worsens risk by allowing unbound oxalate to be absorbed. Uric acid stones are the only type that can be dissolved non-surgically, through urine alkalinisation and urate-lowering therapy. Understanding stone type is therefore essential to moving beyond generic hydration advice.
Kidney Stone Prevention — Fluid Target & Dietary Risk Calculator
Select your stone type, enter body weight and kidney function (eGFR), and optionally your serum uric acid level. The calculator outputs your personalised daily fluid intake target, urine output goal, and stone-type-specific dietary guidance.
⚕ Target urine output ≥2.5 L/day for stone prevention (EAU 2024 guidelines). Fluid intake target = urine output target + insensible losses (~0.5–1.0 L/day for Philippine climate). CKD patients with eGFR <30 may have fluid restrictions — discuss with nephrologist before dramatically increasing fluid intake.
Next Steps
Use the result to support — not replace — clinical judgment.
- Interpret the value against the targets shown in the calculator and the Evidence section below, in the context of the full clinical picture.
- Trend serial measurements rather than acting on a single result; confirm abnormal or unexpected values before changing management.
- Apply the relevant KDIGO / specialty-guideline threshold and document the indication.
- Escalate or refer to nephrology when results are out of range, rapidly changing, or discordant with the clinical picture — and discuss the implications with the patient.
Evidence & References
Formula & Equations
| Parameter | Value / Rule |
|---|---|
| Urine output target — calcium oxalate, calcium phosphate, uric acid, struvite, unknown | ≥ 2.5 L/day (EAU 2024 guideline minimum) |
| Urine output target — cystine stones | ≥ 3.0 L/day (higher solubility threshold required) |
| Fluid intake target (all types, normal eGFR) | Urine output target + 0.8 L/day insensible losses |
| CKD adjustment — eGFR < 30 mL/min/1.73m² | Fluid intake capped at 2.0 L/day; urine output capped at 1.5 L/day — individualize with nephrologist |
| CKD adjustment — eGFR 30–44 mL/min/1.73m² | Standard target maintained; monitor for oedema; aggressive hydration is safe but requires clinical monitoring |
| Elevated serum uric acid (> 6.0 mg/dL) | Additional uricosuric guidance triggered (febuxostat, dietary purine restriction) regardless of stone type |
The 0.8 L/day insensible loss estimate is calibrated for the Philippine tropical climate (ambient temperature 28–35°C, moderate activity). Higher physical activity, fever, or outdoor occupational exposure may increase insensible losses further — the treating clinician should adjust accordingly. Urine colour is the most practical real-time guide: target pale yellow or clearer at all times.
Evidence & References
Fluid intake targets and dietary risk stratification follow the European Association of Urology (EAU) Guidelines on Urolithiasis (2024 edition) and the American Urological Association (AUA) medical management guideline. The 2.5 L/day urine output target is the single most consistent recommendation across international guidelines and meta-analytic evidence. Stone-type-specific dietary interventions derive from randomised controlled trial data (including the seminal calcium supplementation trials) and systematic reviews by Fink et al. and Assimos et al.
- Pearle MS, Goldfarb DS, Assimos DG, et al. Medical management of kidney stones: AUA guideline. J Urol. 2014;192(2):316–324.
- Fink HA, Wilt TJ, Eidman KE, et al. Medical management to prevent recurrent nephrolithiasis in adults: a systematic review for an American College of Physicians Clinical Guideline. Ann Intern Med. 2013;158(7):535–543.
- European Association of Urology. EAU Guidelines on Urolithiasis. EAU Guidelines Office, Arnhem, The Netherlands. 2024 edition.
- Assimos D, Krambeck A, Miller NL, et al. Surgical management of stones: American Urological Association/Endourological Society Guideline. J Urol. 2016;196(4):1161–1169.