- Choose the drug — dapagliflozin (Farxiga) or empagliflozin (Jardiance), the two SGLT2 inhibitors with the strongest CKD and heart-failure evidence.
- Select the primary indication for starting therapy: CKD (albuminuric or progressive), heart failure (HFrEF or HFpEF), or type 2 diabetes for glycemic control.
- Enter the patient's current eGFR (mL/min/1.73 m²).
- Tick on dialysis or type 1 diabetes if applicable — either flag overrides the eGFR logic.
- The result returns the verdict (eligible / do-not-initiate-may-continue / contraindicated), the recommended starting dose, the initiation threshold applied, and a safety-counseling panel.
All computation runs in your browser; no values are stored or transmitted. This is an initiation-and-dose decision aid for clinicians — always confirm against the current label.
When to Use
Use this tool when deciding whether to start dapagliflozin or empagliflozin in an adult with CKD, heart failure, or type 2 diabetes, and at what dose. SGLT2 inhibitors are foundational cardiorenal therapy: KDIGO recommends an SGLT2 inhibitor for most adults with CKD and type 2 diabetes, and for albuminuric or progressive non-diabetic CKD down to the trial eGFR floors. The decision hinges on two things — the indication you are treating and the patient's eGFR relative to that drug's trial-based initiation threshold.
Appropriate population
Adults considered for an SGLT2 inhibitor for cardiorenal protection (CKD or heart failure) or for glycemic control in type 2 diabetes. The eGFR floors differ by drug — empagliflozin initiates from a lower eGFR (≥20) than dapagliflozin (≥25) for CKD and heart failure — so the same patient can be eligible for one agent and not yet the other.
When NOT to use these agents
Do not start an SGLT2 inhibitor in patients on maintenance dialysis (no benefit, contraindicated) or in type 1 diabetes (not indicated; high euglycemic DKA risk). Glycemic efficacy is limited at low eGFR, so for diabetes-glycemia-only indications these agents are not recommended for initiation below the drug's glycemic floor — although the cardiorenal indication, with its lower eGFR threshold, may still apply.
Pearls & Pitfalls
Cardiorenal indication beats the glycemic floor
The "do not initiate below eGFR 45" caveat applies to glycemic efficacy only. For CKD or heart failure, dapagliflozin can be started down to eGFR 25 and empagliflozin down to eGFR 20 — well below the glycemic floor — because cardiorenal benefit persists where glucose-lowering is minimal.
Continue through declining eGFR; the initial dip is expected
Once started, continue the SGLT2 inhibitor until dialysis or transplant even if eGFR falls below the initiation threshold — the benefit persists. Expect a reversible acute eGFR "dip" of roughly 3–5 mL/min in the first weeks; this is hemodynamic, not nephrotoxic, and is not a reason to stop.
Pitfalls
(1) Dialysis → contraindicated; type 1 diabetes → avoid (euglycemic DKA). (2) Hold on sick days and 3–4 days before major surgery (euglycemic DKA risk). (3) Volume depletion / hypotension when combined with loop diuretics — consider down-titrating the diuretic at start. (4) Genital mycotic infections and (rarely) Fournier gangrene — counsel on perineal hygiene. (5) Continue foot care in diabetics. Always confirm the current label for the specific product.
Why Use It
SGLT2 inhibitors are now first-line cardiorenal therapy, but the right answer depends on combining two variables clinicians often handle separately: the eGFR and the indication. The initiation thresholds differ by drug (dapagliflozin ≥25, empagliflozin ≥20 for CKD/HF) and by purpose (glycemic efficacy fades below eGFR ~45, while cardiorenal benefit extends much lower). The common errors are withholding a guideline-recommended agent because eGFR looks "too low" for glycemic control, stopping the drug for the expected initial eGFR dip, or missing the dialysis / type 1 diabetes contraindications. This tool encodes the landmark-trial floors so the start/continue/avoid decision and the dose are explicit.
SGLT2 Inhibitor Eligibility & Dose Check
Choose the drug and indication, enter the eGFR, and flag dialysis or type 1 diabetes. The tool returns the verdict, the recommended starting dose, the initiation threshold applied, and a safety-counseling panel.
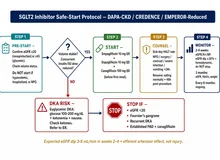
⚕ Decision logic only — no PK math. Initiation eGFR floors: dapagliflozin ≥25 (CKD, HF) and ≥45 for glycemia-only; empagliflozin ≥20 (CKD, HF) and ≥30 for glycemia-only. Standard dose 10 mg once daily (empagliflozin glycemia may use up to 25 mg if eGFR ≥45). Dialysis → contraindicated; type 1 diabetes → avoid. Once started, continue until dialysis/transplant despite eGFR decline. Sources: DAPA-CKD (NEJM 2020), EMPA-KIDNEY (NEJM 2023), DAPA-HF (NEJM 2019), EMPEROR (NEJM 2020), KDIGO 2024 CKD Guideline. Confirm against current product labeling.
Next Steps
Use the verdict to support — not replace — clinical judgment.
- If eligible, start at the recommended dose and counsel the patient on sick-day rules, perioperative holds, genital-infection hygiene, and the expected reversible eGFR dip.
- When co-prescribed with a loop diuretic, reassess volume status and consider down-titrating the diuretic to limit hypotension at initiation.
- If the patient is below the glycemic floor but has CKD or heart failure, reconsider the indication — the cardiorenal threshold is lower and the agent may still be indicated.
- Once started, continue the SGLT2 inhibitor until dialysis or transplant despite a falling eGFR; do not stop for the early hemodynamic dip.
- Document the indication and the eGFR at initiation, and refer to nephrology or cardiology where the picture is complex or discordant.
Evidence & References
Initiation thresholds applied
| Drug | CKD / HF eGFR floor | Glycemia-only eGFR floor | Dose |
|---|---|---|---|
| Dapagliflozin (Farxiga) | ≥ 25 (DAPA-CKD, DAPA-HF, DELIVER) | ≥ 45 (limited glycemic efficacy below) | 10 mg once daily |
| Empagliflozin (Jardiance) | ≥ 20 (EMPA-KIDNEY, EMPEROR-Reduced/Preserved) | ≥ 30 (limited glycemic efficacy below ~45) | 10 mg once daily (up to 25 mg for glycemia if eGFR ≥ 45) |
Once initiated, both agents are continued until dialysis or transplant even if eGFR falls below the floor. Maintenance dialysis is a contraindication; type 1 diabetes is not an indication (high euglycemic DKA risk).
Key safety counseling
| Issue | Action |
|---|---|
| Euglycemic DKA | Hold on acute illness / sick days; hold 3–4 days before major surgery |
| Volume depletion / hypotension | Reassess and consider reducing concurrent loop diuretic at start |
| Genital mycotic infection | Counsel on perineal hygiene; treat early; rare Fournier gangrene |
| Initial eGFR dip | Expected ~3–5 mL/min, reversible — not a reason to stop |
| Diabetic foot care | Continue routine foot surveillance in diabetic patients |
Evidence & References
SGLT2 inhibitors are guideline-recommended cardiorenal therapy. The eGFR initiation floors encoded here come from the landmark CKD and heart-failure trials and the KDIGO 2024 CKD guideline. Glycemic efficacy fades at low eGFR, but cardiorenal benefit extends to the lower trial thresholds, which is why the CKD/HF floors sit below the glycemia floors.
- Heerspink HJL, Stefánsson BV, Correa-Rotter R, et al. Dapagliflozin in Patients with Chronic Kidney Disease (DAPA-CKD). N Engl J Med. 2020;383:1436–1446.
- The EMPA-KIDNEY Collaborative Group. Empagliflozin in Patients with Chronic Kidney Disease. N Engl J Med. 2023;388:117–127.
- McMurray JJV, Solomon SD, Inzucchi SE, et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction (DAPA-HF). N Engl J Med. 2019;381:1995–2008.
- Packer M, Anker SD, Butler J, et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure (EMPEROR-Reduced). N Engl J Med. 2020;383:1413–1424.
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. 2024;105(4S):S117–S314.