- Enter the patient's most recent steady-state eGFR in mL/min/1.73 m² — not a value drawn during acute kidney injury.
- Select whether the patient is not yet started on metformin or is currently taking it — the advice to initiate versus continue differs in the 30–44 band.
- Optionally enter the current total daily dose so the tool can flag dose capping at eGFR 30–44.
- Tick any transient-risk factors present (planned iodinated contrast, acute illness/dehydration/sepsis, decompensated heart failure, hospitalization, before major surgery) — these trigger a temporary hold regardless of the chronic eGFR band.
- Read the verdict card (SAFE / CAUTION / CONTRAINDICATED / TEMPORARY HOLD), the eGFR band, dose advice, monitoring interval, and the lactic-acidosis note.
This is a decision aid, not a substitute for the prescribing information or clinical judgment. All computation runs in your browser; no values are stored or transmitted.
When to Use
Use this checker whenever you are deciding to initiate, continue, dose-cap, hold, or discontinue metformin in a patient with chronic kidney disease, or when a transient event (planned contrast imaging, acute illness, hospitalization, or surgery) raises the question of a temporary hold. The 2023 ADA Standards of Care and the FDA metformin label both define eGFR thresholds: full use at eGFR ≥45, do not initiate (continue with caution and a reduced dose if already taking) at 30–44, and contraindicated below 30.
Appropriate population
Adults with type 2 diabetes and CKD whose steady-state eGFR is known. The eGFR (CKD-EPI, mL/min/1.73 m²) is the threshold variable used by the ADA and the current FDA label — the label was revised in 2016 from a serum-creatinine cutoff to eGFR specifically to allow metformin use in patients with mild-to-moderate CKD.
When NOT to rely on it
Do not apply during acute kidney injury or any non-steady state — use a stable eGFR. This tool addresses the renal safety threshold only; it does not assess hepatic impairment, alcohol use, tissue hypoxia, glycemic adequacy, or other independent metformin contraindications. Always confirm against the current prescribing information and the full clinical picture.
Pearls & Pitfalls
Continue, don't reflexively stop
KDIGO's 2022 Diabetes-in-CKD guideline supports continuing metformin down to an eGFR of 30 in patients with type 2 diabetes and CKD. Metformin is the foundational glucose-lowering agent and overly cautious withdrawal at higher eGFRs leaves patients on less-preferred therapy. The decision changes only when eGFR crosses 45 (do not initiate) and 30 (discontinue).
Cap the dose at eGFR 30–44
If a patient already on metformin drops into the 30–44 band, do not initiate de novo, but continuing is reasonable: reassess the risk/benefit, reduce the total daily dose (commonly capped near 1000 mg/day), and monitor renal function at least every 3 months. Falling below 30 is the discontinuation threshold.
Pitfalls & transient holds
(1) Hold metformin at the time of, or before, iodinated contrast if eGFR <30, or in the eGFR 30–60 range when another risk factor is present; restart 48 h after contrast once renal function is confirmed stable. (2) Hold during acute illness, dehydration, or sepsis and before major surgery — situations that raise lactic-acidosis risk — and resume only when the patient is stable. (3) The rare but serious adverse event is lactic acidosis; counsel patients to stop and seek care for severe nausea, vomiting, myalgia, or malaise. Always confirm against the current label.
Why Use It
Metformin dosing in CKD is a frequent point of clinician hesitation: the older serum-creatinine-based contraindication caused widespread, unnecessary withdrawal, while uncritical continuation below eGFR 30 risks accumulation and lactic acidosis. This checker collapses the current ADA and FDA eGFR thresholds, the KDIGO position, the dose-cap rule for the 30–44 band, and the situational holds (contrast, acute illness, surgery) into a single unambiguous verdict — reducing both inappropriate discontinuation and unsafe continuation.
Metformin Safety Checker in CKD — eGFR-Based Hold / Continue / Discontinue
Enter the patient's steady-state eGFR and current metformin status to get an unambiguous verdict — SAFE, CAUTION, CONTRAINDICATED, or TEMPORARY HOLD — with dose, monitoring, and lactic-acidosis guidance per the 2023 ADA Standards of Care and the FDA label.
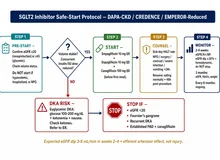
⚕ eGFR thresholds: ≥45 → continue / may initiate, full dose (max ~2000–2550 mg/day); 30–44 → do NOT initiate, continue with caution if already taking, cap dose ≈1000 mg/day, monitor renal function every 3 months; <30 → contraindicated, discontinue. Transient holds (iodinated contrast if eGFR <30 or 30–60 with risk; acute illness/dehydration/sepsis; before surgery) override to a temporary HOLD; restart 48 h after contrast once renal function is confirmed stable. Decision aid only — confirm against the current prescribing information. Source: ADA Standards of Care in Diabetes — 2023, Diabetes Care 2023;46(Suppl 1); FDA metformin label.
Next Steps
Use the verdict to support — not replace — clinical judgment.
- Confirm the eGFR is at steady state before acting; recheck if drawn during acute illness or AKI.
- At eGFR 30–44, document the risk/benefit decision, cap the total daily dose (~1000 mg/day), and schedule renal-function monitoring at least every 3 months.
- For a transient hold, set a clear restart criterion — 48 h after contrast with confirmed stable renal function, or once the acute illness / post-operative state resolves.
- If metformin is stopped or capped, reassess overall glycemic control and consider a complementary agent with cardiorenal benefit (e.g. an SGLT2 inhibitor or GLP-1 receptor agonist), as supported by KDIGO 2022.
- Counsel the patient on lactic-acidosis warning signs and on holding metformin around contrast, acute illness, and surgery.
Evidence & References
Decision logic by eGFR band
| eGFR (mL/min/1.73 m²) | Verdict | Action |
|---|---|---|
| ≥ 45 | SAFE | Continue, or may initiate; full dose (max ~2000–2550 mg/day). |
| 30–44 | CAUTION | Do NOT initiate. If already taking, continue with caution: reassess risk/benefit, reduce dose (cap ≈1000 mg/day), monitor renal function every 3 months. |
| < 30 | CONTRAINDICATED | Discontinue — do not use. |
Transient holds (override to TEMPORARY HOLD)
| Trigger | Action |
|---|---|
| Iodinated contrast imaging | Hold at/before contrast if eGFR <30, or eGFR 30–60 with another risk factor; restart 48 h afterward once renal function is confirmed stable. |
| Acute illness / dehydration / sepsis | Hold — these raise lactic-acidosis risk; resume when the patient is stable. |
| Decompensated heart failure | Hold during decompensation (tissue hypoperfusion / hypoxia risk); resume when compensated. |
| Hospitalization (acute) | Hold during the acute admission; reassess at discharge. |
| Before major surgery | Hold before surgery; resume when oral intake and renal function are stable. |
The rare serious adverse event is lactic acidosis. Counsel patients to stop metformin and seek care for severe nausea, vomiting, myalgia, malaise, or difficulty breathing.
Evidence & References
The 2023 ADA Standards of Care and the current FDA metformin label define metformin's renal safety by eGFR: contraindicated below 30, do not initiate below 45, and a reduced/capped dose with closer monitoring in the 30–44 band. The FDA revised the label in 2016 from a serum-creatinine cutoff to eGFR to allow use in mild-to-moderate CKD. KDIGO's 2022 Diabetes-in-CKD guideline supports continuing metformin down to an eGFR of 30.
- American Diabetes Association. Standards of Care in Diabetes — 2023. Diabetes Care. 2023;46(Suppl 1) — pharmacologic approaches to glycemic treatment and the chronic kidney disease section (eGFR <30 contraindicated; do not initiate at eGFR <45; reduce dose at eGFR 30–44).
- U.S. Food and Drug Administration. Metformin hydrochloride prescribing information — eGFR-based contraindication (<30) and iodinated-contrast hold guidance (2016 label revision).
- Kidney Disease: Improving Global Outcomes (KDIGO) Diabetes Work Group. KDIGO 2022 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease. Kidney Int. 2022;102(5S):S1–S127 — supports metformin to eGFR 30.